Podiatry Weekly is owned and operated by Marat Kazak DPM. All information presented here is for educational purposes only and is not meant to be taken or used as medical advice. Always consult with your doctor before starting or changing your medical therapy or exercise routine. Podiatry Weekly is a participant in the Amazon Services LLC Associates Program and other affiliate programs. We are compensated for referring traffic and business to these companies. We may earn money or products from the companies mentioned in this post.
Anesthesia is a medical technique used to prevent pain and discomfort during surgical procedures. It allows patients to undergo surgery without feeling any pain. Anesthesia helps to keep the patient calm and relaxed during the procedure.
There are several different types of anesthesia that can be used during surgery. This article is about one of the safest and most commonly used Anesthesia for Office procedures: Local Anesthesia.

Coming to the United States from Ukraine at the age of 16, I did not know who I wanted to be. However, I was fascinated by the opportunities offered by the United States education system. In 1997, Ukrainian education system was compromised. Bribes were a common way to advance and get jobs and into educational opportunities. My family would not be able to afford a “good college major”. When we arrived in San Francisco, I quickly learned that the only limiting factor in my education and professional achievement will be me. My success was based on the level of work and energy I was willing to apply.
By late 2000s, I was well on the way to becoming a doctor….
My First Experience with Local Anesthesia
One of the first procedures I had to learn in podiatry school was how to “numb the toe.” This is one of the most common procedures done in podiatry. We, as podiatry students, were given an opportunity to practice on each other under the supervision of an experienced doctor.
I was not sure if I was more afraid of administering the injection or of receiving one.
Before we got on to this experience, we had a full class explaining what local anesthetics are all about. This included how they work, what to expect, exact technique of administration, and how to deal with complications. We all signed waivers and consents for treatment.
I decided that I would like to first administer the injection and then would volunteer and get one, allowing my classmate a chance to practice.
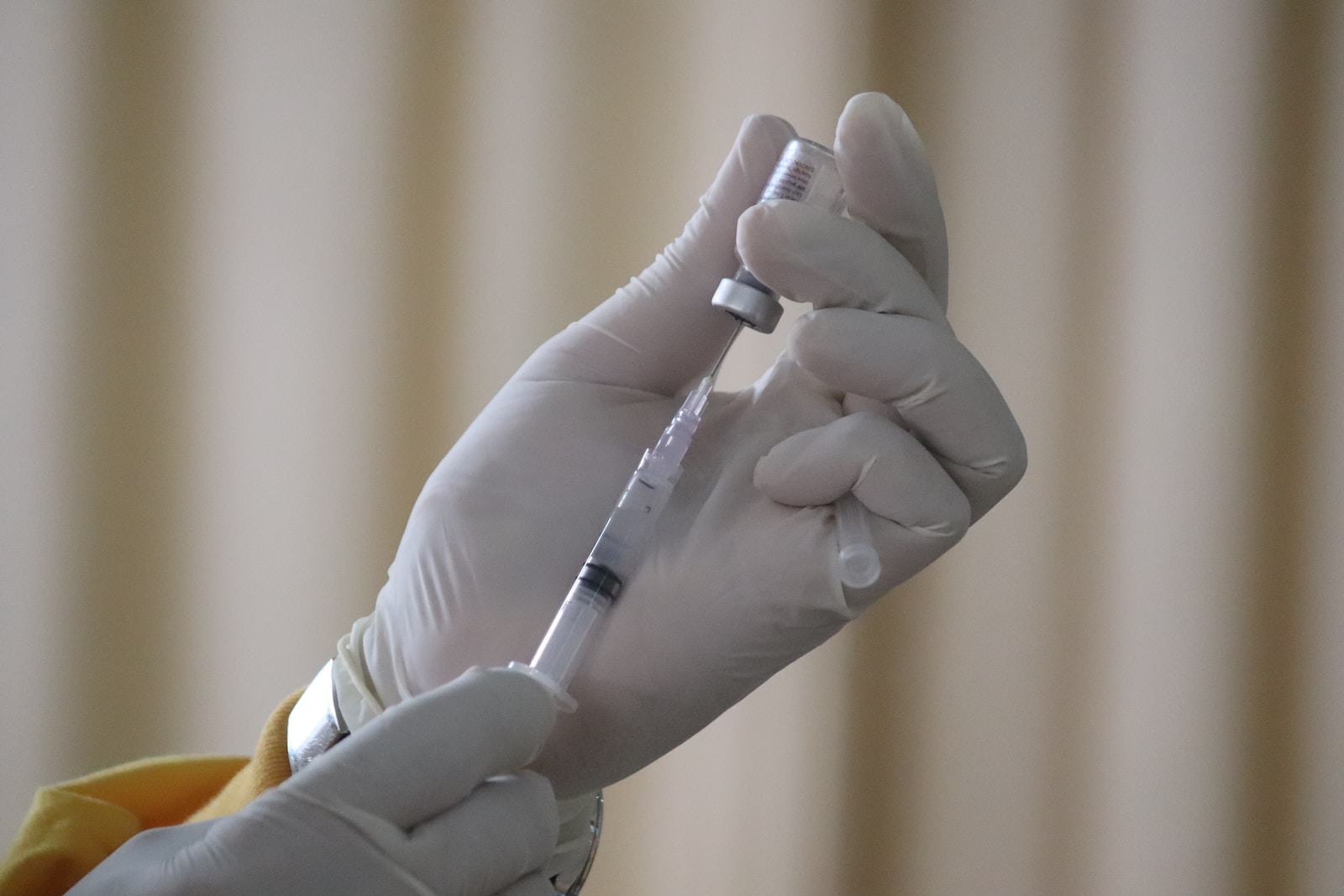
I put on my gloves and cleaned the toe with alcohol solution. I did this by carefully scrubbing it from nail to where it connected on the foot. I drew up local anesthetic in a sterile way mixing short and longer active anesthetic in equal amounts. Another student was helping me. He was spraying a topical anesthetic agent called Ethyl Chloride over the area I was about to pierce with a needle.
I looked at my classmate who was about to get a shot to confirm we are good to go. He nodded in agreement. My assistant started to spray the base of the toe and I was ready with the injection over the skin. As the island of skin about to be injected turned frosty white from the spray, I pierced it with the needle. My volunteer “patient” started to become uncomfortable but indicated I can proceed.
I pulled on the syringe plunger to make sure I am not in the blood vessel. This was confirmed as there was no blood was aspirated. I started the injection. This is when my “patient” really started to become uncomfortable and said that his toe is feeling an intense burn!
For a moment I was conflicted. I was questioning if I am doing something wrong and did not want to hurt my classmate. The doctor supervising the procedure assured us that sensation of burning is normal and instructed me to proceed.
By this time, the anesthetic started to work and numbness helped my patient to feel more at ease. He reported that the burning sensation improved. This was promising and made me feel encouraged. However, I had to do a total toe block. This meant going all around the base of the toe with local anesthetic.
According to the technique I was using at the time, I had to “poke” my patient 3 more times. Neither I nor him were looking forward to this. I was extremely nervous at this point and my classmate just wanted to complete the injection.
I gathered my courage, as I did not want to appear weak in front of my peers. I especially did not want to look weak in front of the supervising doctor. If I could not do this injection, how can I do foot surgery?
Next 3 injections went a bit more predictably. My classmate was happy to get out of the chair with a numb toe.
Now, however, was my turn to get an injection.
My stress level was still very high but I had to play it cool.
I sat into the exam chair and watched my classmate get ready to inject my toe. I was playing out the injection scenario in my mind, as I was getting ready for “poke and burn.”
My heart was racing and my mind was filled with anxiety. I did not want to be in that exam chair. However, I did think it was important for me to have this experience. I was about to learn a lesson that helps me almost every day of my professional life.
As Ethyl Chloride hit my skin, the intense feeling of a cold burn created a distraction from the pain of the needle piercing the skin. The cold burn felt similar in discomfort and intensity to “brain freeze” one feels when eating something very cold. I could not wait for that feeling to go away. Then the needle pierced the skin and the burn started.
I was trying to hold my breath and was trying to be as steady as possible. I closed my eyes and tried to distract myself with thoughts of “happy places.” This did not help.
I started to feel dizzy and nausea kicked in.
I knew this feeling as felt it before.
Prior to starting podiatry school, I worked as medical research assistant at UC Davis Emergency Room.
One day in the ER, I saw a physician stitch patient’s scalp with the patient completely awake. That patient was brought in after a motorcycle accident. Despite the local anesthetic administered around the sculp area, he was in significant discomfort.
Because of the sight of blood and patient’s grimacing, my body went into fight or flight mode. I started to feel dizzy and nauseous and had to step out of the department.
I was angry with myself. My reaction was a reflex and not something I intended to experience. If I could not control how I feel during medical procedures, how could I go into medicine or surgery?
Remembering this episode during my toe injection added to the anxiety.
I felt like I was within seconds of passing out. I had to tell the supervising doctor and my classmate. By this time, he completed injecting my toe.
I told them that I was felt that the room was spinning. I was seeing stars and dark circles and felt like I was about to pass out.
The supervising doctor jumped into action! He told me to take several deep breaths to bring oxygen back to my brain. Holding my breath during the injection likely contributed to my panic response. This helped with the nausea symptoms, but I was still seeing black circles.
They put an ice pack behind my neck and on my forehead. I was instructed to raise my legs about the level of my heart. This was to bring the blood back to the brain. I was given salt of ammonia to breath, as its strong smell was supposed to make me more alert.
Within several minutes, I was feeling well enough to walk around.
This experience taught me valuable lessons on patient safety.
How do I keep my patients safe and comfortable?
I always do procedures with patients reclined in padded exam chairs with no risk of falling. Before doing an invasive procedure like an injection, I place my patient in an exam chair with feet above the heart level. This helps to ensure blood flows to the brain. I encourage the patient to do deep breathing during the injection. Ethyl chloride is used to decrease the sensation of needle prick.
I also do my injections slowly to allow for anesthetic to start working before moving on to next site. My injection technique changed over time. Now, I am usually able to anesthetize the toe with just two needle pricks.
I have started to use an anesthetic buffer to decrease the acidity of the injection agent. This helps to reduce the burning pain sensation.
I speak with my patients during the injection to keep them awake and alert. I also encourage them to communicate with me about what they are experiencing.
Local Anesthesia
The beauty of local anesthesia is in its ability to reduce procedure pain enough to avoid the need for the mind-altering anesthesia. With local anesthesia, you continue to be completely awake and aware. The patient is in full control of body function and decision-making process.
Other types of anesthesia carry increased risk of heart and lung related side effects. These make them potentially less safe in people already struggle with medical ailments effecting those organs.
- Some medical conditions that may pose increased risks include:
Cardiovascular Conditions: Severe heart failure, unstable angina (chest pain), uncontrolled hypertension (high blood pressure), or a recent heart attack may increase the risks associated with general anesthesia.
Respiratory Conditions: Severe chronic obstructive pulmonary disease (COPD), severe asthma, or a history of difficult intubation (insertion of a breathing tube) can make general anesthesia more challenging and increase the risk of complications.
Kidney or Liver Disease: Significant impairment of kidney or liver function may affect the metabolism and elimination of anesthetic agents, potentially leading to complications.
Neurological Conditions: Certain neurological conditions, such as multiple sclerosis (MS), myasthenia gravis, or amyotrophic lateral sclerosis (ALS), may require special considerations during anesthesia due to potential effects on muscle function and respiratory control.
Obesity: Obesity can increase the risks associated with anesthesia, including difficulties with airway management, ventilation, and potential complications related to comorbidities associated with obesity.
Allergies or Drug Reactions: A history of severe allergic reactions to anesthetics or specific medications may influence the choice of anesthetic agents and require alternative approaches.
Pregnancy: Anesthesia during pregnancy requires careful consideration and coordination with the obstetric team to ensure the safety of both the mother and the fetus.
Why it is great for in office use?
Local anesthesia is used to numb a specific area of the body, such as whole foot, an island of skin, or even just a toe. It is often used for minor procedures. For example, numbing the toe to remove an ingrowing nail or to reduce the pain of skin biopsies (cutting out a small fragment of skin for diagnosis of disease). Local anesthesia is usually administered through injections or topical creams, and it takes effect within a few minutes.
Many “minor” procedures can be done with assistance of local anesthetic. Some examples include hammertoe correction, simple bunion correction, wound debridement, and removal of ingrowing nail among others.
Local anesthetics are typically administered through an injection near the site that needs to be numbed. These anesthetics work by temporarily blocking nerve impulses in the area. This prevens the nerves from transmitting pain signals to the brain. Local anesthesia has a relatively quick onset and is generally safe when administered by trained medical professionals.
The effects of local anesthesia are usually limited to the specific area where it is applied. This means that the rest of the body remains unaffected. This makes it different from general anesthesia, which induces a state of unconsciousness.
However, like any medical procedure, it does carry some risks and potential side effects, such as temporary numbness, tingling, or bruising at the injection site.
What are the most commonly used local anesthetics in podiatry?
There are several types of local anesthetics available on the market. The ones most used in podiatry in the United States are Lidocaine and Bupivacaine. They different in duration of anesthesia and onset of action. Lidocaine provides anesthesia in less than a minute and can last, depending on your metabolism, for a few hours. Bupivacaine takes a bit longer to start working but can last from 4 to 12 hours.
Both lidocaine and bupivacaine can be combined with epinephrine.
Why do doctors add epinephrine to local anesthetics?
Epinephrine is a vasoconstrictor, meaning it constricts blood vessels in the area where it is injected.
When added to local anesthetics like lidocaine or bupivacaine, it serves two purposes:
-Prolonging the Anesthetic Effect: Epinephrine helps to slow down the absorption of the local anesthetic into the bloodstream. This prolongs the duration of the anesthetic effect, allowing for longer-lasting pain relief.
-Reducing Bleeding and Enhancing Safety: Epinephrine’s vasoconstrictive properties help to constrict blood vessels in the injection site, reducing bleeding during procedures. This can improve visibility for the healthcare provider and enhance the safety of the procedure
However, your surgeon must be extra meticulous about bleeding control during the procedure that uses epinephrine with local anesthetic. Because of its blood vessel constricting effect, one can miss an injured vessel. This can result in bleeding once epinephrine effect disappears and constriction is reversed.
What can be done to reverse toxic effects of local anesthetic?
Even though local anesthetic use is very safe when used by trained professional, toxicity may occur with excessive doses and accidental introduction of toxic dose into blood stream. Toxicity can be treated with lipid emulsion therapy.
Lipid emulsion therapy, also known as fat emulsion or lipid rescue, is a treatment option that can be used to manage systemic toxicity caused by local anesthetics.
Local anesthetic toxicity occurs when local anesthetic drugs, such as lidocaine or bupivacaine, are inadvertently injected into the bloodstream or absorbed in excessive amounts, leading to systemic effects.
Local anesthetics primarily work by blocking nerve impulses in a specific area, but when they reach high concentrations in the bloodstream, they can affect various organs and systems, including the central nervous system (CNS) and the cardiovascular system. Symptoms of local anesthetic toxicity may include dizziness, confusion, seizures, arrhythmias, cardiovascular collapse, and even cardiac arrest.
Lipid emulsion therapy involves the administration of a lipid emulsion intravenously to help reverse the effects of local anesthetic toxicity.
The lipid emulsion acts as a “sink” for the local anesthetic, sequestering it and reducing its concentration in the bloodstream. The mechanism of action is not completely understood, but it is believed that the lipid emulsion forms a lipid phase that can effectively bind the local anesthetic, preventing it from exerting its toxic effects.
The most used lipid emulsion is Intralipid®, which is a 20% lipid emulsion composed of soybean oil, egg phospholipids, glycerin, and water. It is typically administered intravenously as a bolus followed by a continuous infusion. The dosage and administration regimen may vary depending on the severity of the toxicity and the specific local anesthetic involved.
Lipid emulsion therapy has been shown to be effective in reversing local anesthetic toxicity, especially when used early in the management of severe cases. However, it is important to note that lipid emulsion therapy should be administered by healthcare professionals in a hospital or clinical setting, as it requires careful monitoring and expertise.
In the next series of blogs, I will cover the topics of regional, monitored, and general anesthesia types.
Author bio:
My name is Dr. Marat Kazak. I have been working as a professional Podiatrist serving Northern California community since 2014. My extensive medical and surgical knowledge combined with an ongoing curiosity to learn about the latest trends define my success in the field of foot, ankle and leg medical and surgical care.
If you enjoyed this article, please consider subscribing and sharing!